Panosteitis (Enostosis)
Pathophysiology, Diagnosis, and Management
Panosteitis (sometimes referred to as eosinophilic panosteitis or enostosis) is a spontaneously occurring, self-limiting inflammatory disease of the long bones in young, rapidly growing dogs. While the condition carries an excellent prognosis, the acute, severe nature of the lameness often mimics catastrophic orthopaedic injury, requiring careful diagnostic differentiation.
The disease predominantly affects large and giant breeds between 5 and 18 months of age, with a peak incidence occurring between 5 and 12 months. However, outliers exist, with cases reported in German Shepherd Dogs as young as 2 months and as old as 7 years. Males are affected substantially more often than females. Interestingly, in female patients, the initial clinical episode frequently coincides with their first oestrus.
Aetiology & Pathophysiology
The exact aetiology of panosteitis remains elusive, and a multifactorial origin is highly probable. Historically, viral infections (such as canine distemper or adenovirus) were suspected due to the sometimes concurrent systemic signs like lethargy and fever, though definitive viral isolation has been inconsistent. Modern theories lean toward a combination of genetic predisposition, stress, and high-protein/high-calcium diets promoting rapid growth.
Pathophysiologically, the disease begins with the degeneration of medullary adipocytes (fat cells) within the bone marrow. This triggers intense fibroblastic activity and intramembranous ossification. The resultant vascular engorgement and inflammation within the rigid confines of the bone cortex lead to a dramatic increase in intraosseous pressure. This "compartment syndrome" of the bone is the primary source of the severe pain elicited upon palpation.
Clinical Presentation
The classic presentation is an acute onset of lameness that is unaffected by rest or exercise. The lameness may be marked (sometimes non-weight-bearing) and can last from a few days to several weeks. A hallmark of panosteitis is "shifting lameness" (occurring in approximately 50% of cases), where the disease resolves in one limb only to acutely present in another. Dogs may be completely sound between these bouts, distinguishing it from the persistent lameness seen in other developmental orthopaedic diseases like elbow or hip dysplasia.
Radiographic Staging & The Clinical Disconnect
A critical concept in diagnosing panosteitis is that clinical signs often precede radiographic signs by 1 to 2 weeks. The severity and location of the radiographic lesions do not necessarily correlate with the severity of the clinical pain; the most clinically painful limb may have the least pronounced radiographic changes.
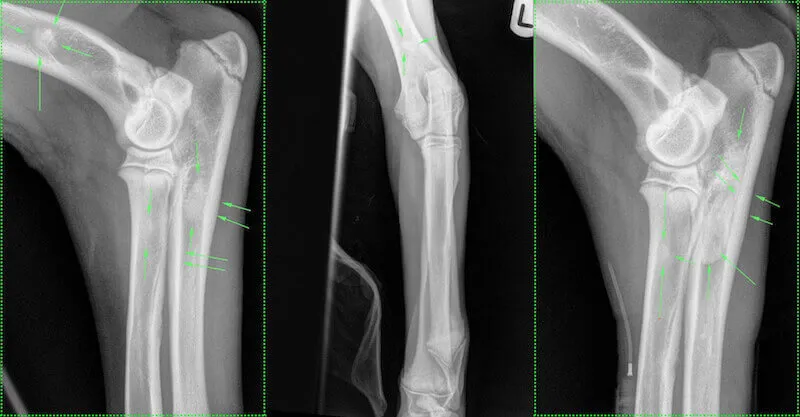
- Early Phase: Changes are subtle. Look for increased radiolucency in the region of the nutrient foramen, followed by a blurring and accentuation of the trabecular pattern. If clinical suspicion is high but radiographs are clean, repeat imaging in 2-3 weeks is advised.
- Middle Phase: Sclerotic radiodensities (nodular, "thumbprint" opacities) appear within the medullary canal, particularly at the proximal and distal ends of the diaphysis. Endosteal and/or periosteal bone proliferation may become evident, thickening the cortex.
- Late Phase: The intramedullary opacities slowly resolve, leaving coarse, thickened trabecular bone. While the medullary canal eventually normalizes, cortical thickening may persist long-term. The complete histological and radiological course in a single bone lasts approximately 90 days.
Differential Diagnosis & Management
Because panosteitis presents in young, growing dogs, the differential diagnosis list is broad. It includes hip and elbow dysplasia, osteochondritis dissecans (OCD), early cruciate disease, and diaphyseal fractures. When shifting lameness is a feature, systemic conditions such as immune-mediated polyarthritis (IMPA), systemic lupus erythematosus, and bacterial endocarditis must be ruled out. The definitive diagnosis relies on the combination of diaphyseal pain on palpation and characteristic radiographic opacities.
Treatment: Because the disease is self-limiting and carries an excellent prognosis for full recovery, treatment is entirely symptomatic. Aggressive pain management is required during acute flare-ups. NSAIDs and opioids are the mainstays of therapy and should be utilized in preference to corticosteroids. Exercise restriction during acute bouts helps limit concurrent soft tissue inflammation.
Selected References
- Brinker, Piermattei, Flo et al. Handbook of Small Animal Orthopaedics and Fracture Repair, Fifth Edition.
- Bojrab JM, Waldron DR, Toombs JP. Current Techniques in Small Animal Surgery, Fifth Edition.
- Thrall DE. Textbook of Veterinary Diagnostic Radiology, Sixth Edition.
- Fossum T. Small Animal Surgery - 4th Edition.
- Slatter D. Textbook of Small Animal Surgery, Third Edition.
- Houlton JEF, Cook JL, Innes JF, Langley-Hobbs SJ. BSAVA Manual of Canine and Feline Musculoskeletal Disorders.