Metaphyseal Osteopathy (HOD)
Clinical Review, Diagnostic Imaging, and Evidence-Based Management
Metaphyseal osteopathy (MO), traditionally referred to as Hypertrophic Osteodystrophy (HOD), is a developmental, auto-inflammatory bone disease affecting young, rapidly growing large and giant breed dogs. The age of onset typically falls between 7 weeks and 8 months, with peak incidence clustered strictly between 3 and 4 months of age.
While diagnosed in over 40 breeds, profound genetic predispositions exist in Weimaraners, Irish Setters, Great Danes, Boxers, and German Shepherds. Familial clustering in entire litters of Weimaraners and Australian Kelpies underscores a strong heritable component. The disease is characterized by profound, acute-onset neutrophilic inflammation within the metaphyses of the long bones, leading to necrosis, micro-fracturing of trabecular bone, and severe clinical lameness.
Pathogenesis: The Autoinflammatory Paradigm
The etiology of MO was historically attributed to hypovitaminosis C; however, this has been thoroughly disproven, and Vitamin C supplementation is contraindicated as it may exacerbate dystrophic calcification. Current evidence points to a complex, heritable immune dysregulation.
Recent serological studies in affected Weimaraners and Irish Setters have demonstrated significantly elevated innate immunity cytokines (IL-1β, IL-6) during active disease, classifying MO alongside human autoinflammatory bone disorders like CRMO (Chronic Recurrent Multifocal Osteomyelitis). Furthermore, temporal associations with modified-live canine distemper virus (CDV) vaccinations have been heavily documented, suggesting the vaccine acts as an immunological trigger in genetically susceptible phenotypes.
Clinical Signs & Systemic Manifestations
The cardinal sign is an acute onset of severe, bilateral lameness. Physical examination reveals exquisitely painful, warm, and swollen distal metaphyses of the radius, ulna, and (less commonly) the tibia. Metaphyseal swelling must be carefully differentiated from joint effusion during palpation.
MO frequently presents with profound systemic illness. Patients often exhibit marked pyrexia, lethargy, and anorexia. In severely affected individuals—particularly Weimaraners—the systemic inflammatory response syndrome (SIRS) can manifest with hematochezia, purulent ocular/nasal discharge, pustular dermatitis, and potentially fatal pneumonia.
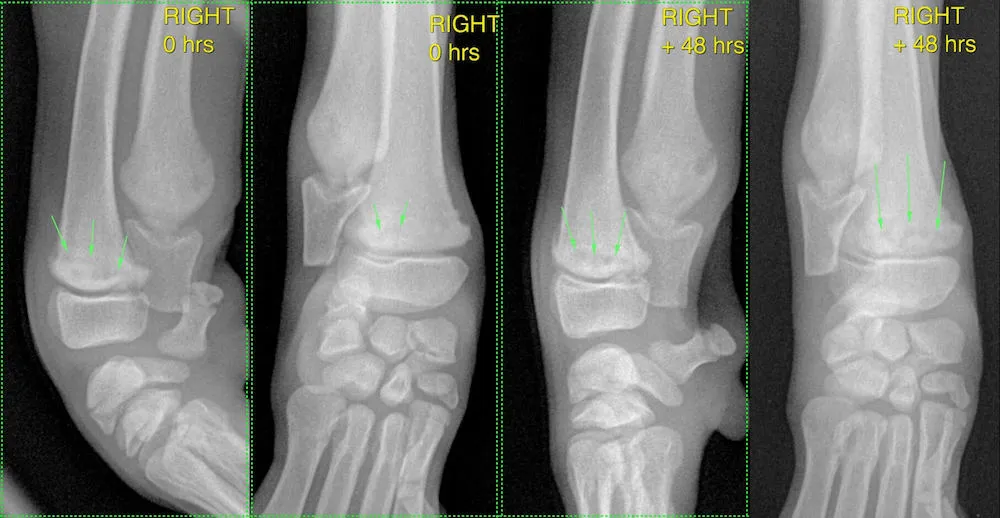
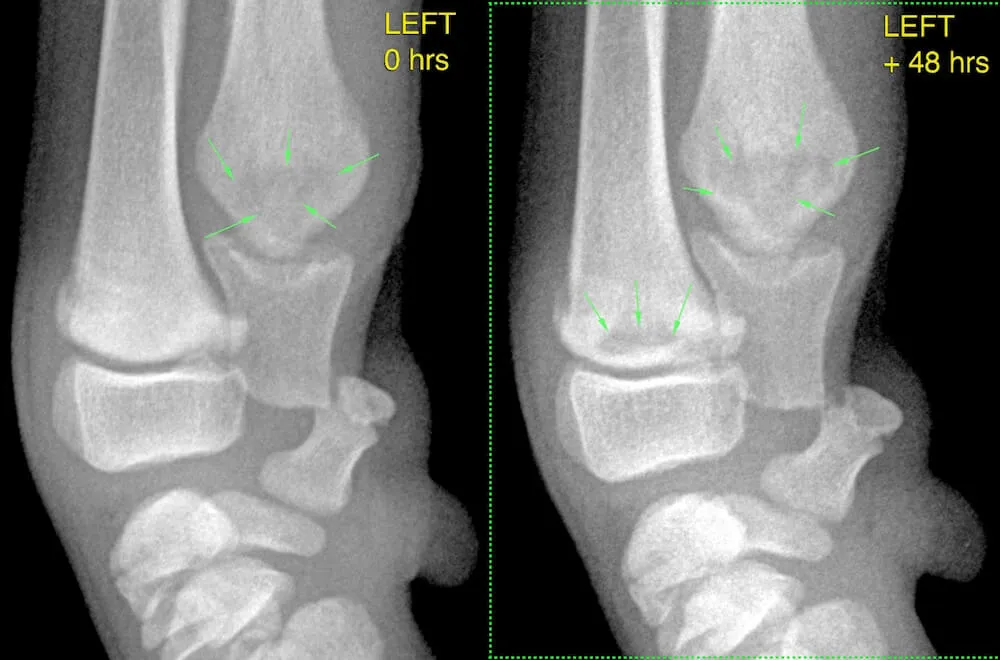
Diagnostic Imaging: The "Pseudophysis"
Radiography remains the diagnostic gold standard. The initial pathognomonic sign is an irregular, transverse radiolucent band located in the metaphysis, running parallel to the physis (the "pseudophysis"). This lucency represents an area of suppurative necrosis and trabecular micro-fracturing.
This zone is often bordered by a thin margin of subchondral bone sclerosis caused by the collapse of necrotic trabecular bone. As the disease progresses chronologically, extensive subperiosteal new bone formation (cuffing) occurs along the metaphyseal cortices. In severe or relapsing cases, premature physeal closure may occur, resulting in complex angular limb deformities (e.g., radius curvus).
Evidence-Based Treatment Protocols
Treatment is primarily supportive, aimed at controlling the severe inflammatory cascade and managing hyperalgesia. IV crystalloid therapy is required for patients with severe pyrexia and anorexia.
Standard Therapy: For most breeds exhibiting mild to moderate MO, non-steroidal anti-inflammatory drugs (NSAIDs) combined with multimodal analgesia (e.g., opioids, gabapentin) are the first line of defense. The disease is typically self-limiting.
The Corticosteroid Exception: A landmark retrospective study evaluating treatment responses in Weimaraners fundamentally altered clinical guidelines. Safra et al. (2013) demonstrated that 54.5% of Weimaraners failed to respond to NSAID therapy. Conversely, 100% of the Weimaraners treated with immunosuppressive doses of corticosteroids exhibited dramatic clinical resolution within 8 to 48 hours. Consequently, in patients presenting with peracute, severe systemic illness—particularly Weimaraners—immunosuppressive corticosteroid therapy (e.g., Prednisone at 1-2 mg/kg/day, tapered over 4-6 weeks) is now considered the standard of care. True bacterial osteomyelitis or physitis must be ruled out prior to initiation.
References & Clinical Citations
- Safra N, Hitchins PL, Maverakis E, et al. (2016). Serum levels of innate immunity cytokines are elevated in dogs with metaphyseal osteopathy during active disease and remission. Veterinary Immunology and Immunopathology.
- Safra N, Johnson EG, Lit L, et al. (2013). Clinical manifestations, response to treatment, and clinical outcome for Weimaraners with hypertrophic osteodystrophy: 53 cases (2009–2011). Journal of the American Veterinary Medical Association, 242(9): 1260–1266.
- Greenwell CM, Brain PH, Dunn AL. (2014). Metaphyseal osteopathy in three Australian Kelpie siblings. Australian Veterinary Journal, 92: 115–118.
- Abeles V, Harrus S, Angles JM, et al. (1999). Hypertrophic osteodystrophy in six Weimaraner puppies associated with systemic signs. Veterinary Record, 145: 130–134.
- Harrus S, Waner T, Aizenberg N, et al. (2002). Development of hypertrophic osteodystrophy and antibody response in a litter of vaccinated Weimaraner puppies. Journal of Small Animal Practice, 43: 27–31.