Medial Compartment Disease (MCD)
Pathophysiology, Radiographic Triage, and Dynamic Unloading
From ED to DED
Historically, "Elbow Dysplasia" (ED) was utilized as an umbrella term encompassing four distinct conditions: Ununited Anconeal Process (UAP), Osteochondritis Dissecans (OCD) of the humeral condyle, Fragmented Medial Coronoid Process (FMCP), and joint incongruity.
Modern veterinary orthopaedics has largely abandoned this blanket terminology in favour of Developmental Elbow Disease (DED). This shift acknowledges that these conditions are not always isolated entities but are frequently interconnected manifestations of underlying biomechanical and developmental abnormalities—most notably, radioulnar incongruity (RUI) and trochlear notch dysplasia.
Similarly, the term "Fragmented Medial Coronoid Process" (FMCP) has been superseded by Medial Coronoid Disease (MCD). This reflects the clinical reality that the medial coronoid process does not simply "fragment" spontaneously. Instead, it undergoes a spectrum of disease ranging from microcracking and chondromalacia to complete fragmentation, driven by chronic mechanical overload.
The Paradigm Shift: From FCP to MCD
For decades, Canine Elbow Dysplasia—specifically Fragmented Medial Coronoid Process (FMCP)—was conceptually managed as a simple intra-articular fracture. The historical standard of care relied on the superficial arthroscopic removal of the fragmented cartilage and bone, often yielding frustratingly variable long-term functional results.
Modern veterinary orthopaedics has catalyzed a paradigm shift. We now recognize this condition not as an isolated fragment, but as a complex syndrome of radioulnar incongruity (RUI), trochlear notch dysplasia, and dynamic mechanical overload. Broadly classified as Medial Compartment Disease (MCD), the pathology is driven by supraphysiologic weight-bearing forces acting on the medial coronoid, which bears approximately 60% of the transarticular load. Consequently, surgical management has evolved from simple debridement to aggressive subchondral therapy and biomechanical load-shifting osteotomies.
Diagnostic Triage: The Power of Subchondral Sclerosis
While Computed Tomography (CT) is widely regarded as the gold standard for mapping complex 3D incongruity and highlighting occult coronoid fissures, the absence of a CT scanner should not delay definitive surgical intervention.
Non-displaced fissures and micro-fragmentation of the medial coronoid process are notoriously invisible on standard orthogonal radiographs due to the superimposition of the radial head. However, Wolfe's Law dictates that bone remodels in response to mechanical stress. The secondary biomechanical consequences of MCD are highly visible, predictable, and diagnostically robust on standard 2D films.
Ulnar Trochlear Notch Sclerosis: The Trigger for Arthroscopy
Chronic mechanical overload of the medial compartment predictably leads to increased bone density (sclerosis) deep to the articular surface. On a high-quality, perfectly positioned flexed lateral radiograph, subchondral sclerosis of the ulnar trochlear notch presents as an area of increased radiopacity that loses the normal trabecular pattern, often appearing as a solid white "moon crescent" deep to the joint space.
This sclerotic change—even in the complete absence of visible osteophytosis or a discrete bone fragment—carries a remarkably high positive predictive value for MCD. The presence of this sclerosis alongside a compatible clinical presentation (front leg lameness, joint effusion, pain on elbow extension/supination) is entirely sufficient clinical justification for immediate diagnostic and therapeutic arthroscopy.
Therapeutic Arthroscopy & SCO
The transition toward Subtotal Coronoidectomy (SCO) was driven by histological evidence demonstrating that the bone beneath the fragmented cartilage is inherently diseased. Osteomalacia, microcracks, and fatigue fractures extend deep into the trabecular bed of the coronoid process. Leaving this diseased bone intact guarantees continued microfracturing and persistent arthralgia.
SCO involves the aggressive arthroscopic removal of the craniolateral portion of the medial coronoid process, utilizing an arthroscopic burr or osteotome to resect down to healthy, bleeding subchondral bone. This removes the mechanically incompetent bone and encourages the formation of a fibrocartilaginous scar capable of withstanding load.
- Efficacy Data: Retrospective studies indicate that 70% to 75% of dogs treated with SCO prior to 12 months of age show significant early clinical improvement.
- The Ceiling Effect: Because SCO treats the local lesion but does not alter the overarching joint geometry or cure underlying RUI, force-plate analyses show up to 45% of limbs continue to exhibit microscopic lameness long-term, and radiographic osteophytosis invariably progresses.

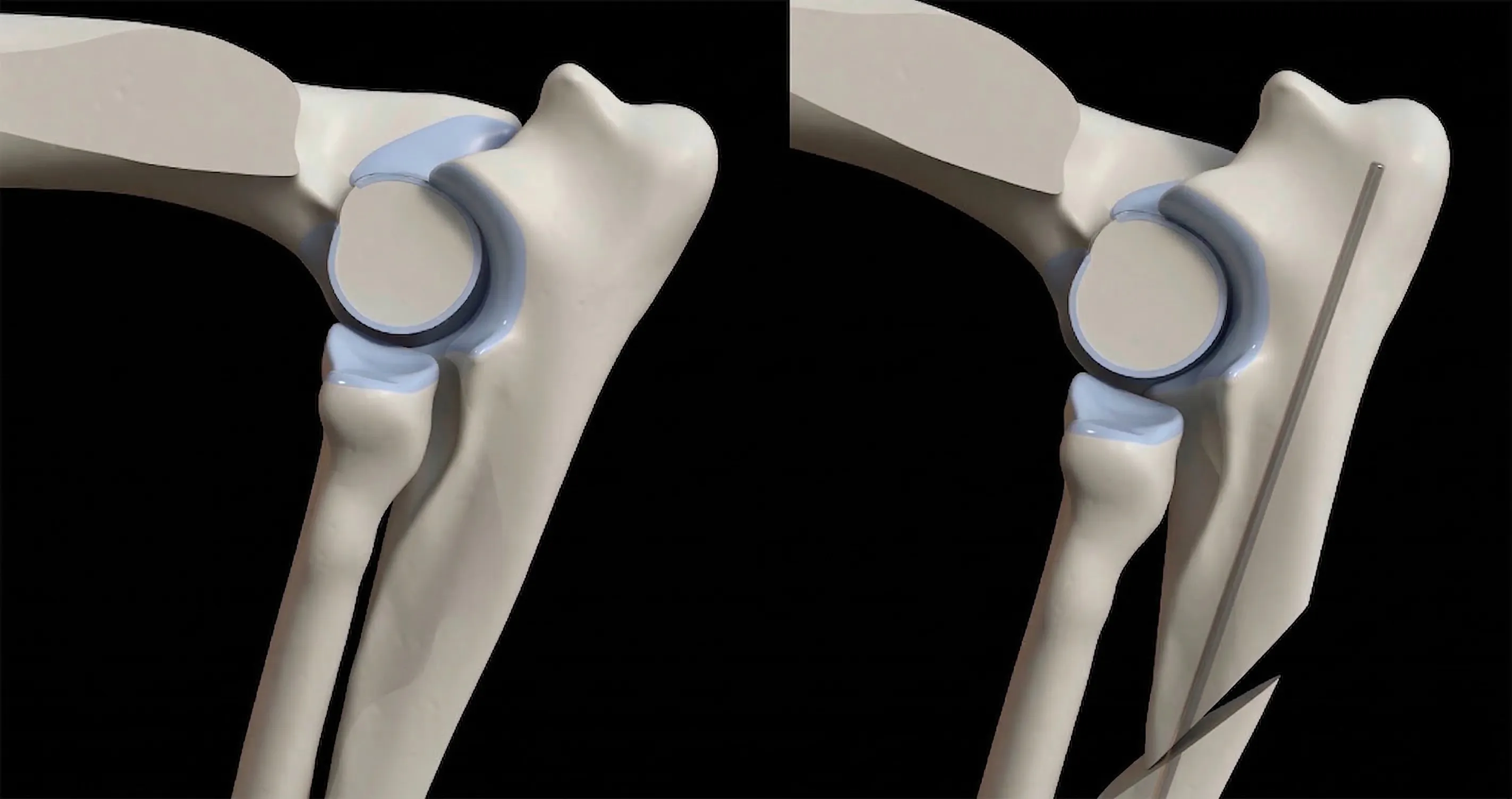
 Top: Fissured coronoid. Bottom: SCO reaching bleeding subchondral bone.
Top: Fissured coronoid. Bottom: SCO reaching bleeding subchondral bone. Addressing Incongruity: Adjunctive Osteotomies
When profound cartilage erosion (Modified Outerbridge Score III-IV), severe RUI, or extensive apical coronoid lesions are identified via arthroscopy, SCO alone is insufficient. The literature robustly supports combining SCO with mechanical unloading procedures to shift the weight-bearing axis laterally, away from the collapsing medial compartment.
PAUL (Static Unloading)
The Proximal Abducting Ulnar Osteotomy (PAUL) uses a specialised, stepped ALPS titanium plate to physically induce a static valgus shift. By forcibly altering the anatomical axis of the ulna, it unloads the medial compartment.
- Outcomes: ~70–75% of owners report improved function at 12 months.
- Complication Profile: Major complications (10–15%) are heavily tied to the hardware, including implant failure, delayed union, and surgical site infections requiring eventual plate removal.

BODPUO (Dynamic Unloading)
The Bi-Oblique Dynamic Proximal Ulnar Osteotomy (BODPUO) utilizes a precise caudo-cranial and latero-medial cut, freeing the proximal ulna to dynamically seek a congruent position without rigid hardware constraints.
- Outcomes: Kinetic studies demonstrate significant increases in Peak Vertical Force (PVF) by 6 months, matching or exceeding static techniques. Radiographic union is robust by 12–16 weeks.
- Complication Profile: Distinctly lower major complication rates (< 5%) due to the absence of rigid fixation plates, virtually eliminating hardware-associated infections.
The BoneVet Clinical Perspective
At BoneVet, our surgical planning is strictly guided by current evidence and a commitment to minimizing patient morbidity. For the management of advanced Medial Compartment Disease accompanied by RUI or severe cartilage loss, our preferred adjunctive procedure is the Bi-Oblique Dynamic Proximal Ulnar Osteotomy (BODPUO) performed concurrently with arthroscopic SCO.
The inherent brilliance of BODPUO lies in its dynamic nature. Rather than forcing the joint into a static, pre-calculated realignment using heavy hardware (as seen in PAUL), BODPUO relies on the physiologic forces of the triceps mechanism and the interosseous ligament to naturally settle the ulna into its path of least resistance. This successfully unloads the medial compartment while respecting the unique mechanics of the individual patient.
Furthermore, the substantially lower complication profile—specifically the elimination of hardware-associated morbidities and catastrophic implant failures—makes BODPUO a significantly safer, highly reliable, and cost-effective intervention for our primary care partners and their clients.
Prognosis and Collaborative Management
While arthroscopic intervention prior to 12 months of age yields clinical improvement in roughly 70% of cases, CED remains a progressive, lifelong osteoarthritic condition. We rely heavily on our primary care partners to facilitate long-term multimodal osteoarthritis management (NSAIDs, joint supplements, weight control, and physiotherapy) post-discharge to maximize surgical outcomes.
Selected Clinical References
- Burton, N.J., et al. (2007). "Reliability of radiological assessment of ulnar trochlear notch sclerosis in dysplastic canine elbows." Journal of Small Animal Practice.
Validates subchondral sclerosis as a highly predictive, independent indicator of MCD on standard orthogonal radiographs, justifying arthroscopic exploration. - Fitzpatrick, N., Yeadon, R. (2009). "Working algorithm for treatment decision making for developmental disease of the medial compartment of the elbow in dogs." Veterinary Surgery.
Establishes the modern framework for combining subchondral debridement (SCO) with dynamic and static unloading osteotomies based on compartment pathology. - Vezzoni, A., et al. (2014). "Arthroscopic findings in 182 elbows with medial coronoid disease." Veterinary Surgery.
Details the varying histopathology of the subchondral bone, confirming that surface cartilage removal is insufficient, thereby necessitating SCO. - Caron, A., et al. (2023). "Clinical and radiographic outcomes of bi-oblique dynamic proximal ulnar osteotomy in dogs with medial compartment disease." Veterinary and Comparative Orthopaedics and Traumatology.
Demonstrates the kinematic efficacy and profoundly lower complication rate of BODPUO compared to static plating techniques.